Vesicoureteral reflux (VUR)
What is vesicoureteral reflux?
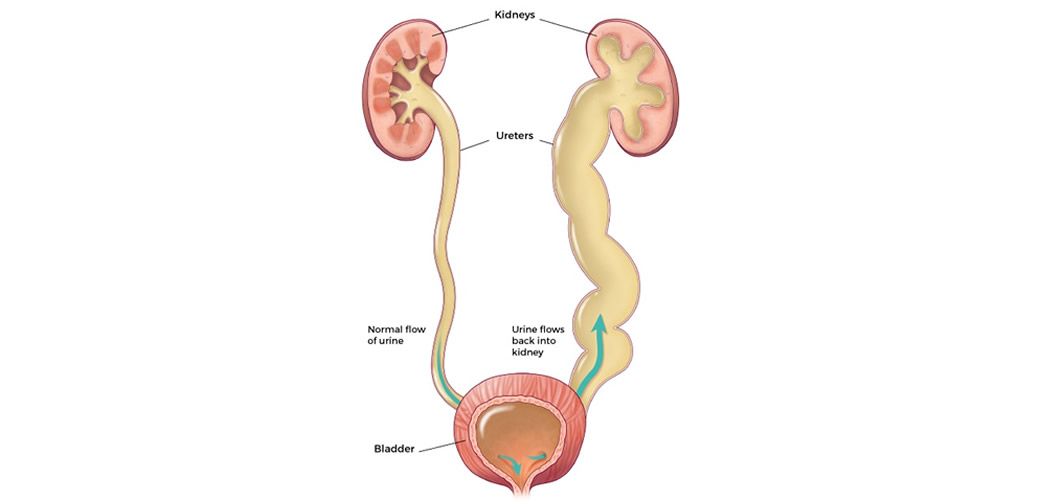
Urine is formed in the kidneys. Under normal conditions, urine flows in one direction: from the kidney down the ureter into the bladder. Vesicoureteral reflux (VUR) occurs when urine returns from the bladder through the ureter to the kidney. This reverse movement of the urine can be on one side or both sides.
Why does VUR occur?
VUR often represents a congenital anomaly. It occurs when the connection between the bladder and the ureter is not good. The lower part of the ureter passes through the bladder muscle. If this joint is too short or shifted to the side, VUR may occur. This is called the primary VUR. In addition, VUR can also occur when the bladder, for some reason, does not function normally but generates high urine pressure, which at some point makes urine return to the kidney. This is the so-called secondary VUR.
What indicates that a child has a VUR?
VUR can be suspected already during pregnancy when ultrasound detection of enlargement of the renal pelvis of the fetus is detected. Such a finding warrants additional testing at birth. Otherwise, the most common VUR is diagnosed if a child develops a urinary tract infection.
What are the symptoms of a urinary tract infection?
Urinary infection is usually the first sign to arouse suspicion of one of the anomalies of the urological tract, including VUR. Symptoms and signs of urinary infection in children, unlike adults, can be very nonspecific. The smaller the child, the less specific the symptomatology, and may manifest as:
- High body temperature
- Irritability
- Loss of appetite
- Frequent urination
- Urgency for voiding
- Burning sensations during urination
- Change in urine color and odor
- Fever
How is a VUR diagnosed?
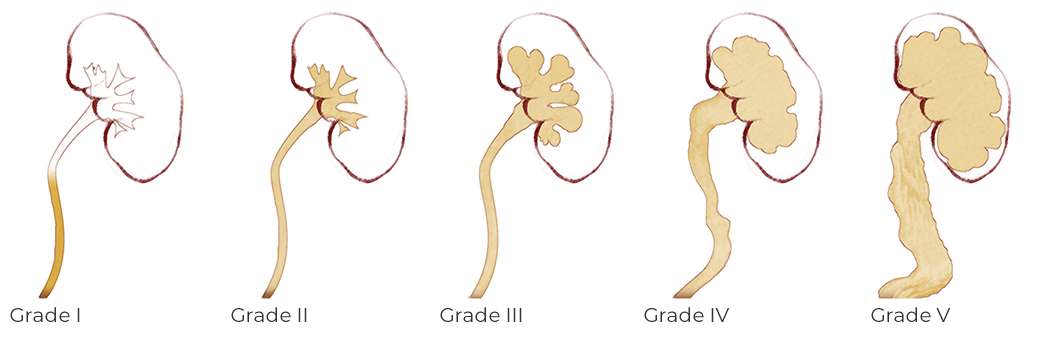
VUR can be suspected if ultrasound shows enlargement of the ureter or renal pelvis. The diagnosis of VUR requires the so-called cystourethrography or MCUG. It is the imaging of the urinary tract with X-rays using a special color (contrast). If a VUR is present, this test also shows its degree. There are five degrees of VUR.
There is now also a diagnostic method for VUR that avoids X-ray radiation, called ultrasound micturating cystourethrography. A special solution is administered into the bladder that is visualized on a special ultrasonic device. It is also possible to determine the degree of VUR by this method.

Is VUR Dangerous?
Based on the recording, your doctor will tell you how serious your child's VUR is on a scale from I (mild) to V (severe). Mild forms of VUR most often resolve by themselves. On the other hand, the more severe the VUR, the less likely it is to withdraw. The consequences of VUR can be very serious. Kidney infection can occur if the child has a urinary tract infection and the infected urine returns to the kidneys. These infections can lead to scarring and damage to the kidney, causing a decrease in kidney function and high blood pressure later in life. VUR in the most severe cases can lead to complete and permanent failure of the kidney.
How is VUR treated?
It is important to treat VUR to prevent possible kidney infection and damage. There are 3 options for the care and treatment of VUR.
- Antibiotics can be used to prevent infections until the VUR has receded on its own. This therapy can take several years and the child must take the medicine daily. These children must be regularly tested for VUR. Antibiotics are best suited for milder forms of VUR. Sometimes long-term antibiotic treatment can lead to bacterial resistance, leading to new infections.
- Endoscopic treatment - the "gold standard" in the treatment of VUR, and is performed by injecting endopaste to the place where the ureter enters the bladder. Kids usually go home the same day.
- Operation - the so-called ureteral reimplantation aims to correct ureteral defects and stop VUR. Most children are cured with this surgery. Surgery is the method of choice in children who have not been successfully treated with endoscopic treatment or who have associated ureteral or bladder anomalies.
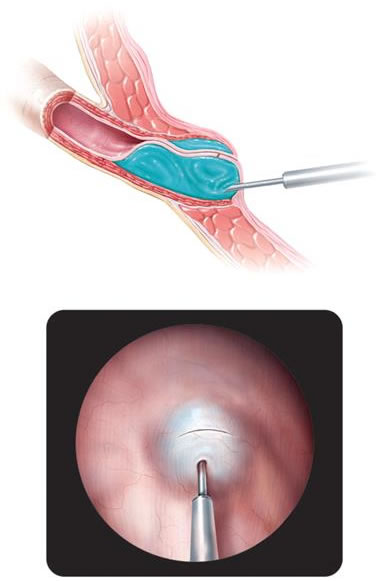
What does endoscopic intervention look like?
The endopaste (gel) is placed in the body where the ureter enters the bladder. This prevents urine from returning to the ureters and the kidneys. After some time, new tissue is formed around the gel providing long-term results. During the intervention, a small camera, a cystoscope (one type of an endoscope used to inspect the bladder) is used to accurately position the gel. During this procedure, the child is under general anesthesia. There is usually no pain after the procedure. The baby may feel a slight tingling sensation during the first few urinations. In most of the times the child goes home the same day. This procedure is minimally invasive, safe and offers excellent results, even with the treatment of high grade reflux.
Picture gallery
These pictures may be inappropriate for you!